AbbVie has been staging a generational handoff for years: as Humira’s U.S. exclusivity fell and biosimilars swarmed, the company groomed Rinvoq and Skyrizi as the next standard-bearers. Investors already know the script: AbbVie has guided the duo to more than $31 billion in combined sales by 2027, and Humira’s 2022 global peak north of $21 billion is now a reference point, not a forecast. The company has announced the first head-to-head trial of TNF-inhibitor cycling versus switching to a JAK inhibitor. The result? Rinvoq beat Humira on both low disease activity and remission at 12 weeks in RA patients who had failed a prior TNF.
AbbVie has been staging a generational handoff for years: as Humira’s U.S. exclusivity fell and biosimilars swarmed, the company groomed Rinvoq and Skyrizi as the next standard-bearers. Investors already know the script: AbbVie has guided the duo to more than $31 billion in combined sales by 2027, and Humira’s 2022 global peak north of $21 billion is now a reference point, not a forecast. The company has announced the first head-to-head trial of TNF-inhibitor cycling versus switching to a JAK inhibitor. The result? Rinvoq beat Humira on both low disease activity and remission at 12 weeks in RA patients who had failed a prior TNF.
Rinvoq pulls ahead in RA trial
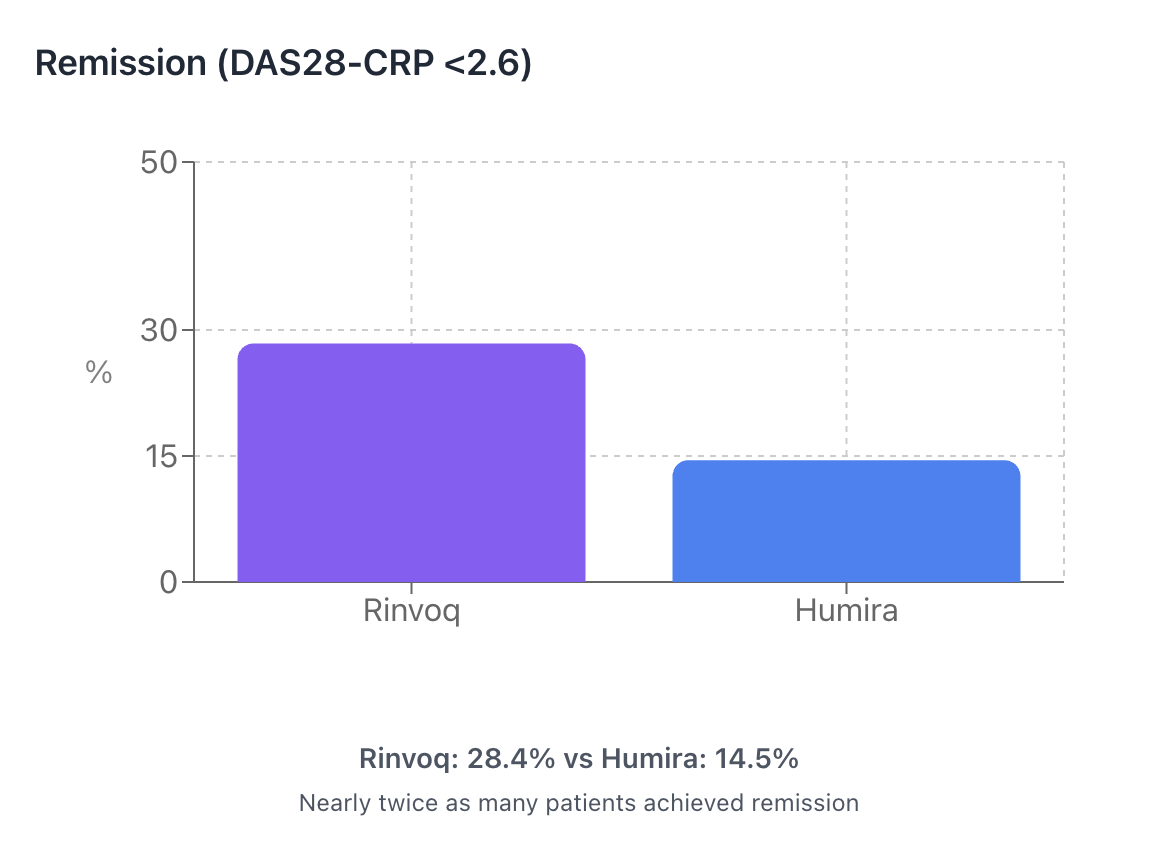
In the Phase 3b/4 SELECT-SWITCH study, patients with RA who had failed or couldn’t tolerate one TNF inhibitor (a class of drugs that blocks tumor necrosis factor, a key inflammatory protein) were randomized to either switch drug classes to the JAK inhibitor Rinvoq, which works by blocking different inflammatory signals inside cells, or to “cycle” to another TNF inhibitor, Humira. At 12 weeks, Rinvoq pulled ahead: 43.3% of patients reached low disease activity (minimal joint swelling and pain) versus 22.4% on Humira; 28.4% hit remission (essentially symptom-free) versus 14.5%. The trial is the first head-to-head comparing these two strategies, and the 12-week safety snapshot showed no new risks, with a blinded extension still tracking patients. Full results are headed to a journal and medical congress.
 The data could potentially drive more payer support
The data could potentially drive more payer support
The results challenge a common insurance hurdle. Many health plans use step-therapy, requirements that patients try cheaper drugs first, and rebate deals that have historically pushed patients to cycle through multiple TNF inhibitors after the first one fails, even as lower-cost biosimilars entered the market. A randomized win for switching drug classes gives clinicians hard data to argue against that automatic TNF-to-TNF cycling. The open question: will pharmacy benefit managers (PBMs) update coverage based on this efficacy evidence, or keep defaulting to whichever option delivers the best rebate?
There are safety caveats. Twelve weeks is short to catch rare but serious events. Rinvoq carries JAK-class boxed warnings, the FDA’s strongest alert, for risks including major adverse cardiovascular events (heart attack, stroke), blood clots (venous thromboembolism), and cancer. Those warnings emerged from post-market studies and led to restricted use in older patients and those with cardiovascular risk factors. Humira’s label warns chiefly of serious infections and malignancy, backed by decades of real-world use. Longer follow-up matters. Second, the trial measured disease activity with DAS28-CRP, a score that includes C-reactive protein, an inflammation marker. Because JAK inhibitors directly suppress CRP, they can look better on CRP-based scales than on other remission criteria that don’t rely on that lab value, so it’s worth watching how Rinvoq performs on alternative measures in the full dataset.
Ultimately, SELECT-SWITCH could give AbbVie what the Rinvoq launch needed: head-to-head proof that switching drug mechanisms after TNF failure works better than cycling within the same class. Treatment guidelines from rheumatology societies already endorse mechanism-switching as a strategy, but insurance coverage policies haven’t caught up. The question is whether PBMs will respond to efficacy data or keep anchoring decisions to price and rebate flow.
Filed Under: Biologics