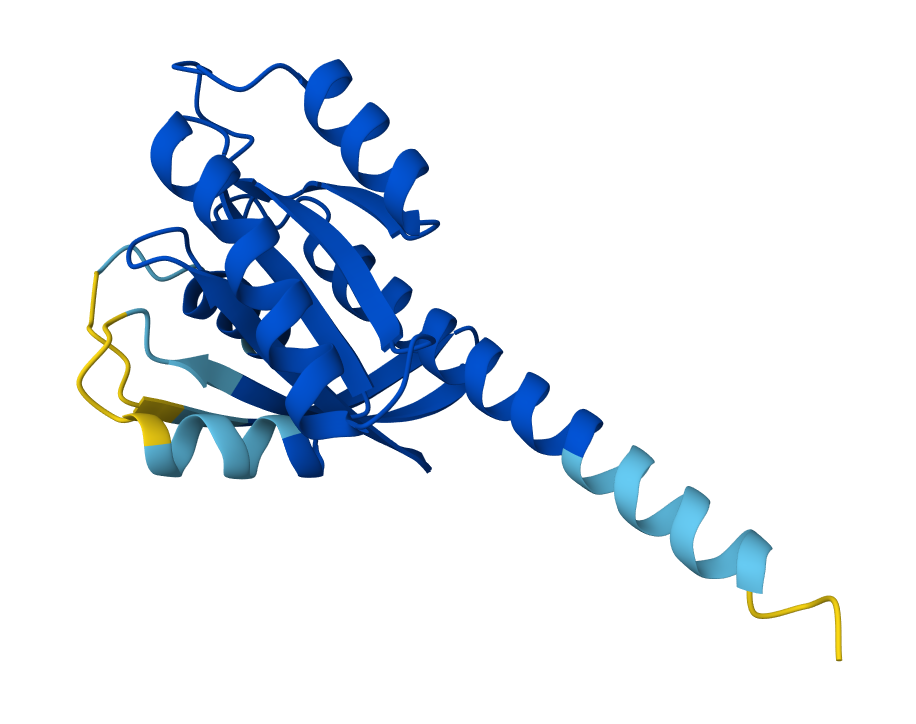
Input configuration for predicting the human KRAS G12C mutant in complex with the inhibitor Sotorasib (AMG 510) using AlphaFold 3.
Biotech is heating up again. The SPDR S&P Biotech ETF (XBI) has gained roughly 69% over the past year. Global life sciences M&A hit $240 billion in 2025, an 81% jump from the prior year, with EY reporting a record $2.1 trillion in deal capacity. Goldman Sachs expects broader M&A volume to rise sharply in 2026.
“It really wasn’t until Q4 of last year that we started to see a rebound,” said Dr. Christiana Bardon, Managing Partner of MPM BioImpact, a Boston-based biotech investment firm that manages roughly $3 billion and focuses on building companies from founding through public markets. “I’m hoping we’re seeing the return of the generalist investor to the biotech sector.”
“We had one of our portfolio companies, Aktis Oncology, go public in January, and it was 18x oversubscribed,” she added. “That tells you how much demand there is for a high-quality, top-class asset priced appropriately.”
Capital, however, is flowing disproportionately to clinical-stage, de-risked assets. J.P. Morgan tracked just 50 seed and Series A investments worth $2.3 billion in Q1 2026, down from 60 investments totaling $3.7 billion a year earlier, putting first-time biotech financings on pace for their worst year since before the pandemic. And large pharma companies cut more than 22,000 jobs in 2025, with the cuts continuing into the first half of this year.
Even as the industry sheds headcount, the money that remains is concentrating in oncology, which now accounts for more than a quarter of biotech venture investment by deal value (roughly 32%, up from 23% in 2020). That focus is on full display this week as the field converges on Chicago for the 2026 ASCO Annual Meeting, the world’s largest oncology conference. Three storylines stand out: a RAS inhibitor that nearly doubled median overall survival in previously treated metastatic pancreatic cancer, overall survival data for a Chinese-developed bispecific that could challenge Merck’s $32 billion Keytruda franchise, and a wave of acquisitions betting that cell therapy can move from specialized academic centers to ordinary clinics.
A RAS inhibitor nearly doubles survival in pancreatic cancer

Dr. Chris Bardon
For decades, the RAS family of oncogenes drove roughly 90% of pancreatic cancers while remaining stubbornly resistant to drug development, earning the moniker “undruggable.” That changed in April, when Revolution Medicines reported that daraxonrasib, an oral RAS(ON) multi-selective inhibitor, nearly doubled median overall survival in previously treated metastatic pancreatic cancer: 13.2 months versus 6.7 months for standard chemotherapy (HR 0.40, p < 0.0001) in the Phase 3 RASolute 302 trial. The drug received FDA Breakthrough Therapy Designation, and full results will be presented in an ASCO plenary session on May 31. The work builds on foundational research by UCSF’s Kevan Shokat, who first identified a druggable pocket on mutant KRAS in 2013, and Frank McCormick, who led the NCI’s RAS Initiative.
Scientists have long called KRAS the “greasy ball,” Bardon explained, because the protein is hydrophobic with no obvious pockets for a drug to bind to. “We’ve never had a breakthrough before in pancreatic cancer; all we’ve had is mostly failure and very incremental contributions,” she said. “It’s kind of like in lung cancer when we figured out EGFR therapies and developed drugs like Tagrisso.”
A molecule that caught pharma off guard
Over the past decade, PD-1 inhibitors became the backbone of cancer immunotherapy, generating more than $50 billion in combined annual revenue. Now a molecule developed in China may be poised to supplant them. Ivonescimab, a bispecific antibody that simultaneously blocks PD-1 and VEGF, is advancing through a series of global Phase 3 trials. Summit Therapeutics submitted a BLA for ivonescimab in EGFR-mutated NSCLC, which the FDA accepted for filing in January 2026 with a PDUFA date of November 14, 2026. At ASCO 2026, overall survival data from the Phase 3 HARMONi-6 trial, comparing ivonescimab plus chemotherapy against a PD-1 inhibitor plus chemotherapy in first-line squamous NSCLC, will be presented in a plenary session.
“I don’t think I would have invested in a company starting this kind of molecule because we had no idea it would work,” Bardon said. “It was only because these drugs are generating clinical data very easily in China that we saw the data and were literally floored.”
If the HARMONi-6 overall survival data are positive, Bardon argues, the implications extend well beyond lung cancer: because ivonescimab has already shown strong progression-free survival data against a PD-1-based regimen, with the key overall survival test coming at ASCO, it may prove superior across many of the indications PD-1 inhibitors are currently approved for. She pointed to this year’s AACR pharma partnering event as evidence the industry already sees that possibility. “Last year, when the ivonescimab data first hit, nobody had a PD-1/VEGF in their pipeline. Surprise, surprise, this year they do,” she said. “If this trial is positive, no pharma company, especially ones with PD-1s like Merck and BMS, can afford not to have a PD-1/VEGF.”
What comes after a $32 billion franchise loses exclusivity
As for Merck & Co., the company’s Keytruda franchise now includes Keytruda Qlex, a subcutaneous formulation of pembrolizumab approved in September 2025 that can be administered in as little as one minute (versus 30 minutes for IV infusion) across 38 solid tumor indications. Together, the IV and subcutaneous versions generated $31.7 billion in 2025. The drug’s core U.S. patent expires in 2028, making it the largest single patent cliff event in pharmaceutical history. The Qlex formulation is classic lifecycle management: migrate prescribers to a new, patent-protected version before biosimilars can launch against the original IV formulation. At least seven companies, including Samsung Bioepis, Sandoz, Celltrion, and Amgen, are developing pembrolizumab biosimilars, with FDA submissions expected as early as this year. Merck CEO Rob Davis has framed the transition as manageable: “I’m quite confident that we will be in a position at a minimum to go through a very shallow period post the LOE, returning in a few years to growth.”
But the competitive threat may not come from biosimilars alone. Analysts at RBC Capital Markets wrote in April that “market optimism is building” that ivonescimab’s results “could lead to accelerated FDA approval and begin to erode Merck’s dominance in first-line lung cancer.”
“The LOE will dramatically affect Merck because of the huge revenue that drug generates,” Bardon said. “But the next chapter of that drug may be PD-1/VEGF. Imagine $60 billion of aggregate revenue across all PD-1s, and now imagine that all being replaced with a new drug targeting PD-1/VEGF. That’s why this is so huge.”
Making cell therapy ordinary
Keytruda Qlex turned a 30-minute infusion into a one-minute injection. For the nearly 200,000 Americans diagnosed each year with blood cancers, including leukemia, lymphoma, and myeloma, the field’s most potent therapy remains far harder to deliver.
Traditional CAR-T cell therapies can produce durable remissions in blood cancers, but the manufacturing process is slow, expensive, and confined to specialized centers. Eli Lilly paid up to $2.4 billion in February to acquire Orna Therapeutics, a company using engineered circular RNA paired with lipid nanoparticles to generate CAR-T cells inside a patient’s body, designed to eliminate the need to extract and re-engineer cells in a lab. Orna is the latest in a string of in vivo CAR-T acquisitions, following AbbVie’s $2.1 billion purchase of Capstan Therapeutics, BMS’s $1.5 billion acquisition of Orbital Therapeutics, and AstraZeneca’s $1 billion deal for EsoBiotec.
The field has moved through three chapters, according to Bardon. Personalized autologous CAR-T can cure patients, but the cost is high, manufacturing is slow, and only sophisticated academic medical centers can administer it. Allogeneic cell therapy using donor cells, the second chapter, “turned out to be very difficult and not very effective,” she said. That pushed the field directly to chapter three: programming cells inside the body. MPM BioImpact was an investor in Orna before the Lilly acquisition. “They use lipid nanoparticles to deliver circular RNA to a cell and make it a CAR-T inside the patient,” Bardon said. “This is utterly transformative because it would be off-the-shelf and could be used by community physicians.”
Filed Under: Oncology