Merck didn’t design calderasib to be the most potent KRAS G12C inhibitor on its own. It was designed to be the most combinable inhibitor.
The KRAS gene encodes a protein that signals for cell growth. It cycles between active and inactive states, signaling when cells should divide. Although it is one of the most commonly mutated genes across human cancers, it was considered undruggable for decades due to its smooth surface.
The G12C mutation locks KRAS in its active state, but it also creates a small binding groove to which drugs can covalently attach. First-generation KRAS G12C inhibitors, such as sotorasib and adagrasib, trapped KRAS G12C in its inactive state. But this mechanism only worked on the fraction of KRAS molecules that happened to cycle into the inactive state. In cancer cells, most KRAS molecules stay in the active state.
“Because KRAS is such an important protein involved in so many cellular processes, resistance to these medications happens quickly and is quite common, since there are a lot of overlapping pathways that interact with KRAS,” explained Jane Healy, vice president and head of oncology early development at Merck Research Laboratories.
Merck designed its inhibitor to solve this problem, while keeping combinability in mind. “We designed it to be highly specific to mutant KRAS, thereby minimizing interaction with the wild-type version and reducing toxicity, but we also designed it with combinability in mind,” said Healy.
Tracking response through the blood
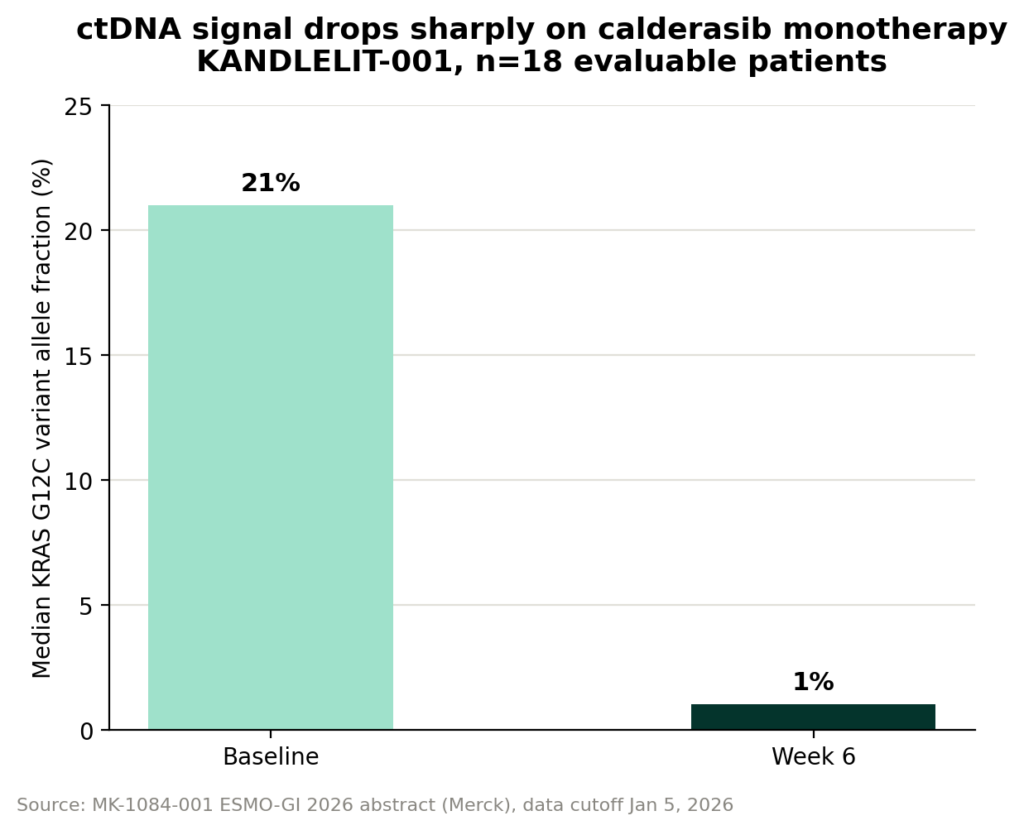
To measure how Merck’s inhibitor, calderasib, decreases the KRAS G12C variant allele fraction, the fraction of circulating tumor DNA carrying the G12C mutation, researchers collected ctDNA, tumor DNA fragments shed into the bloodstream via a blood draw. This was measured at several points throughout the treatment in the KANDLELIT-001 Phase 1 trial.
VAF serves as the biomarker for tumor burden because it indicates fewer mutant tumor cells circulating and shedding DNA. When tumors grow, VAF rises, sometimes even before it’s visible on a scan.
“If you track the KRAS G12C variant allele fraction over the course of treatment, it declines, and we can track that across all patients in the study,” said Healy. “The reduction in variant allele fraction in the blood correlates quite nicely with the responses we’re seeing by imaging.”
In the monotherapy arms, calderasib reduced VAF by a median of approximately 95%, dropping from 21% at baseline to 1% at week 6. However, this is based on only 18 ctDNA-evaluable patients.
Healy told Drug Discovery and Development that the same VAF-response correlation extends across the full study population, including the combination arms, though those figures were not included in the written abstract and are expected to be detailed in the live presentation.
Measuring VAF via blood draws is broadly understood to be faster, cheaper and less burdensome than measuring tumor burden via imaging. VAF opens the door to more frequent monitoring between scans, potentially flagging resistance or progression earlier than imaging would allow.
However, VAF is a relative fraction, not an absolute measure of tumor burden. It can be influenced by how much total ctDNA is shedding, not just how much is mutant DNA.
The tumor-agnostic pembrolizumab approval
The biomarker-first approach is not new to Merck; the company has built an entire regulatory strategy around it before.
“Merck actually had the first tumor-agnostic approval for a drug, with pembrolizumab, through our KEYNOTE-158 program… That was the first tumor-agnostic biomarker approval for a drug,” Healy said.
That trial used microsatellite instability-high (MSI-High) status, a marker for deficient mismatch repair genes. Patients with that biomarker status had a higher response rate relative to patients without it, and this was consistent across a number of different tumor types. Merck also drew on retrospective data from confirmatory pembrolizumab trials and saw the same pattern.
Pembrolizumab has since gained a second tumor-agnostic approval based on tumor mutational burden. “So it’s now a precedented approach, and we’re proud to have been first to use that strategy,” Healy said.
The company is turning to the tumor-agnostic approach again with calderasib. “We have a study looking at calderasib activity across tumor types — any patient with a KRAS G12C-mutated solid tumor can enroll — taking a biomarker-driven approach rather than a tumor-type-specific one,” Healy said.
Patients who have a KRAS G12C-mutated solid tumor, regardless of organ of origin, qualify for the study. The pan-tumor study relies on the same logic as the pembrolizumab trial, focusing on treating mutation status, not tissue of origin. It’s a strategy the company has now applied twice, on two different drugs, nearly a decade apart, suggesting a durable approach to development rather than a one-time regulatory maneuver.
Whether that same biomarker-first logic pays off for calderasib the way it did for pembrolizumab will depend on data still to come.
Testing the combinability thesis
But that biomarker-first philosophy is only as credible as the data behind it. The numbers from KANDLELIT-001 are the most direct test to date.
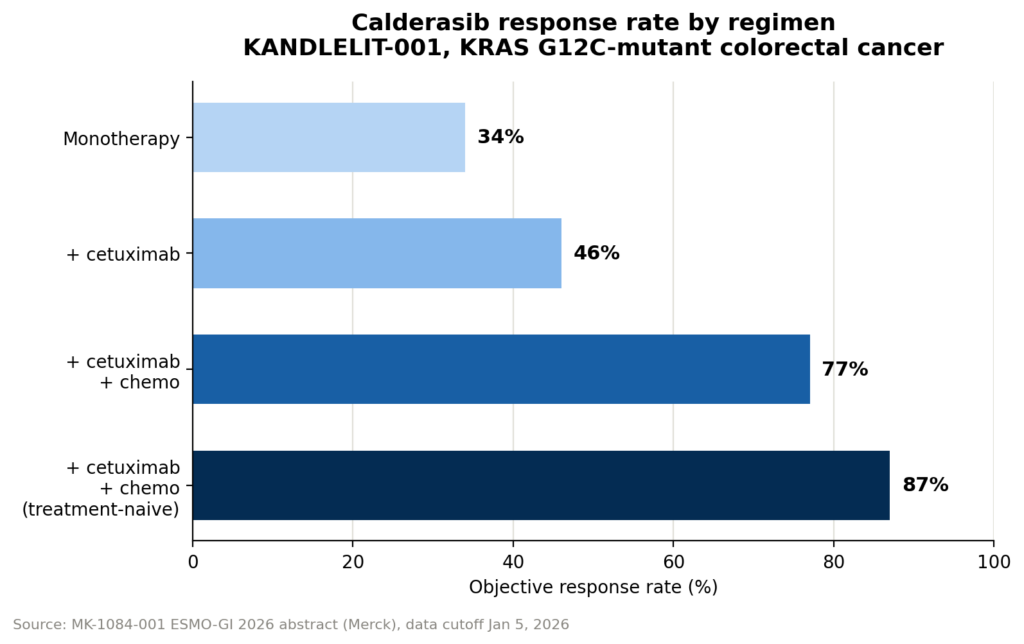
Calderasib by itself has an objective response rate (ORR) of 34%, but in combination with cetuximab, this rises to 46% and in combination with cetuximab and chemotherapy, it reaches 77%. Among patients who hadn’t yet received any prior systemic therapy, the triplet’s response rate climbed even higher, to 87%.
The drug by itself is also well tolerated, but the combination regimens cause more adverse effects. Only 9% of patients experienced grade 3 or 4 drug-related adverse effects on calderasib alone, but this rises to 20% in the doublet arm and 42% in the triplet arm.
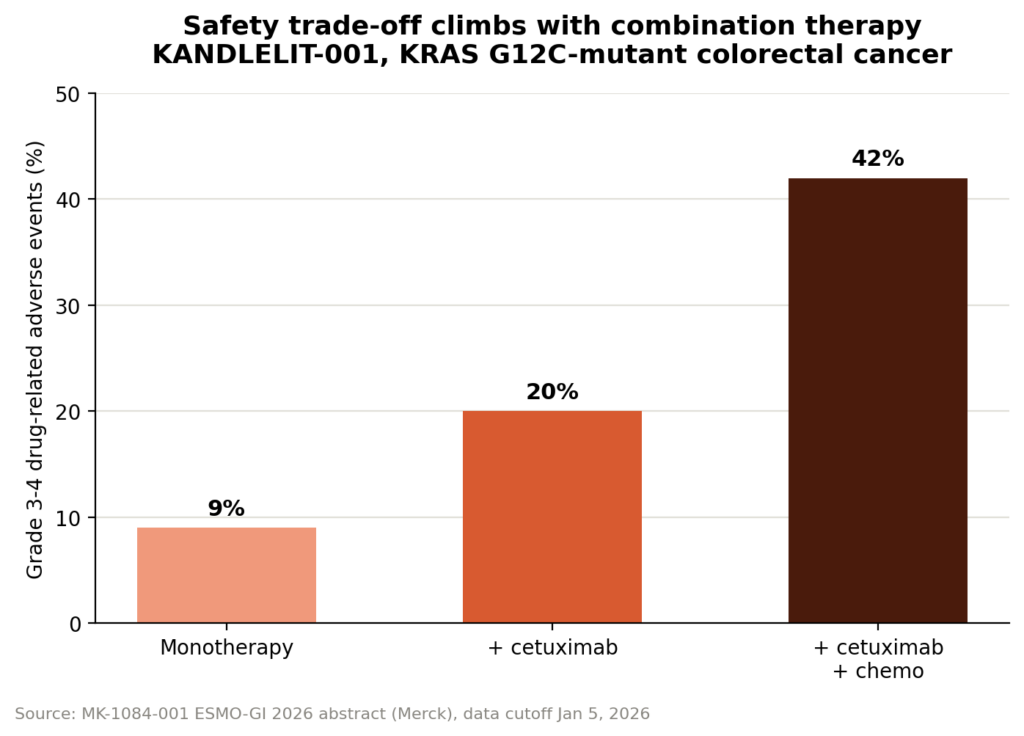
Still, “the combination appears manageable and reflective of the profiles of those individual agents,” Healy said.
This was a relatively small, non-randomized dataset, so future trials will be more revealing and reliable.
The Phase 3 KANDLELIT-012 trial will evaluate calderasib with cetuximab and chemotherapy in 1L KRAS G12C-mutant CRC.
Filed Under: Oncology